Objective: To evaluate the clinical efficacy of combined cystoscopy and laparoscopy for vesicovaginal fistula repair in a single position. Methods: A retrospective analysis was conducted on the clinical data of 6 patients with vesicovaginal fistula treated in the Department of Urology, The First Affiliated Hospital of Jinan University from August 2017 to November 2023. All patients underwent a single-position cystoscopy combined with laparoscopic vesicovaginal fistula repair. Intraoperatively, the fistula was localized transurethrally via cystoscopy, and place ureteral stents. Simultaneously, laparoscopic repair of the fistula was performed via abdominal approach. Recording Surgical duration, intraoperative blood loss, length of hospital stay, intraoperative complications and postoperative complications. Results: All 6 patients underwent successful repair without conversion to open surgery. Operative time was 263.5±49.6 min, intraoperative blood loss was 35.0±20.7 ml, hospital stay was 15.5±5.4 days. At follow-up ranging from 3 to 12 months, no patients developed complications such as urinary leakage, and postoperative quality of life showed significant improvement. Conclusion: Combined cystoscopy and laparoscopy for vesicovaginal fistula repair in a single position avoids multiple repositioning, offering advantages such as simplified technique, short operative time, minimal trauma, and reducedloss blood. This approach represents a safe and effective therapeutic modality.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Vesicovaginal Fistula Repair, Laparoscopy, Cystoscopy, Single Position, Modified Lithotomy Trendelenburg Position
1. Introduction
A vesicovaginal fistula (VVF) refers to an abnormal passage formed between the bladder and vagina. Clinically, it primarily manifests as uncontrolled, persistent leakage of urine from the vagina, which may be accompanied by vaginal wetness, foul odor, and lower urinary tract symptoms. VVF is one of the most common types of acquired fistulas, often secondary to obstetric or gynecological surgical injuries and radiotherapy for pelvic malignancies
[1]
Shrestha DB, Budhathoki P, Karki P, Jha P, Mainali G, Dangal G, Baral G, Shrestha M, Gyawali P. Vesico-Vaginal Fistula in Females in 2010-2020: a Systemic Review and Meta-analysis. Reprod Sci. 2022; 29(12): 3346-3364.
. Reports indicate the incidence rate of obstetric fistula among women of childbearing age is 0.29‰ while the incidence rate among newly pregnant women is 0.09‰
[2]
Adler AJ, Ronsmans C, Calvert C, Filippi V. Estimating the prevalence of obstetric fistula: a systematic review and meta-analysis. BMC Pregnancy Childbirth. 2013; 13: 246.
. The incidence rate of VVF following hysterectomy is approximately 1.0‰
[3]
Duong TH, Taylor DP, Meeks GR. A multicenter study of vesicovaginal fistula following incidental cystotomy during benign hysterectomies. Int Urogynecol J. 2011; 22(8): 975-979.
. Due to its high incidence according to the global disease burden data published by the World Health Organization, VVF has become a public health issue
[4]
Wall LL. Obstetric vesicovaginal fistula as an international public-health problem. Lancet. 2006; 368(9542): 1201-1209.
Persistent vaginal leakage not only predisposes patients to recurrent urinary tract infections, compromising their physical health, but also significantly impacts their psychological well-being, family relationships, and sexual life, severely diminishing quality of life
[5]
Ahmed S, Holtz SA. Social and economic consequences of obstetric fistula: life changed forever?. Int J Gynaecol Obstet. 2007; 99 Suppl 1: S10-S15.
. Conservative management proves ineffective for most VVF patients, necessitating surgical intervention
[6]
Oakley SH, Brown HW, Greer JA, et al. Management of vesicovaginal fistulae: a multicenter analysis from the Fellows' Pelvic Research Network. Female Pelvic Med Reconstr Surg. 2014; 20(1): 7-13.
. Approaches include transvaginal, transabdominal, and transvesical techniques. The transabdominal approach is the second most common method for surgical treatment of VVF, encompassing open, laparoscopic, and robot-assisted laparoscopic techniques. Among these, laparoscopic VVF repair adheres to the fundamental principles of transabdominal repair while reducing recurrence rates and improving cosmetic outcomes. Offering advantages such as enhanced visualization, minimal trauma, and reduced blood loss, it has emerged as one of the primary surgical techniques for transabdominal VVF repair in recent years
[7]
Nesrallah LJ, Srougi M, Gittes RF. The O'Conor technique: the gold standard for supratrigonal vesicovaginal fistula repair. J Urol. 1999; 161(2): 566-568.
However, the currently prevalent laparoscopic VVF repair approach for typically involves first performing cystoscopy in the lithotomy position to identify the fistula and ureteral orifice locations, followed by placement of a ureteral stent. The patient is then repositioned to either the supine position or a Trendelenburg posistion before proceeding with laparoscopic VVF repair. This approach necessitates intraoperative repositioning, requiring hasby two rounds of surgical position preparation and draping, thereby increasing risks associated with prolonged operative time presenting room for improvement. Based on this, our department refined the technique by performing cystoscopy combined with laparoscopy for vesicovaginal fistula repair under a single position. This technique employs a modified low lithotomy position with a 25°Trendelenburg tilt. On the perineal side, perform cystoscopy to locate the fistula, place ureteral stents and complete other procedures. Simultaneously, perform laparoscopic repair of VVF on the abdominal side. Compared to the commonly used two-position laparoscopic VVF repair technique, performing cystoscopic-laparoscopic combined VVF repair in a single position avoids multiple changes in surgical positioning. This approach facilitates better localization of the fistula and protection of the ureter, shortens the operative time, and to some extent reduces the incidence of intraoperative ureteral injury. Between August 2017 and August 2024, our department treated 6 patients with VVF. All six patients underwent single-position cystoscopy combined with laparoscopic vesicovaginal fistula repair, achieving satisfactory outcomes. The findings are reported below.
2. Materials and Methods
2.1. General Data
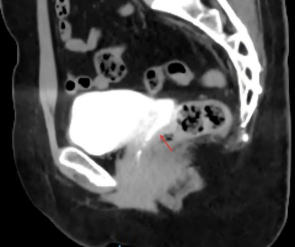
We reviewed the clinical records of 6 patients with vesicovaginal fistula admitted to our department between August 2017 and August 2024. The mean age was 51.33 ± 4.50 years. Five cases resulted from total hysterectomy (3 cases of cervical cancer, 1 case of uterine fibroids, and 1 case of endometrial hyperplasia), while 1 case resulted from neoadjuvant radiotherapy for cervical cancer. All patients had a disease course exceeding 3 months from the onset of vaginal urine leakage to the present surgery, and all underwent primary repair. Preoperative confirmation of VVF was achieved through physical examination, methylene blue test, cystoscopy, and CT urography (CTU), ruling out other possible urinary fistulas such as ureterovaginal fistula. Cystoscopy was used to determine the location, number, size, and distance from bilateral ureteral orifices to the fistula. All 6 patients had single fistula opening located above the bladder trigone and on the posterior-inferior bladder wall. The mean diameter of the fistula openings was 1.8 ± 0.8 cm, and the distance from both ureteral orifices was >1.0 cm. Patients with a history of malignant tumors routinely underwent biopsy of the fistula orifice to rule out neoplastic lesions.
Figure 2. Use cystoscopy to determine the location, number, size of VVF.
2.2. Surgical Procedure
Preoperative Preparation: Routine urine analysis was performed preoperatively to control urinary tract infection, with urine tests repeated until essentially normal. Vaginal cleansing with diluted povidone-iodine solution was administered 3 days prior to surgery. Preoperative fasting was required for 6 hours, with fluid restriction for 4 hours.
Following endotracheal intubation and induction of general anesthesia, position the patient in a modified lithotomy position with the feet elevated. Perform routine perineal and abdominal disinfection and draping. Perform cystoscopy to reconfirm the location, size, and number of fistula openings, as well as their relationship with both ureters and the bladder neck. Place an 5 Fr ureteral stent within the fistula tract as an intraoperative marker. Under wire guidance, examine both ureters and place an 5 Fr ureteral stent to prevent intraoperative injury. The vagina was irrigated twice with diluted povidone-iodine solution and packed with povidone-iodine gauze to prevent air leakage during laparoscopic manipulation. One assistant remained at the perineal side to operate the cystoscope, assisting subsequent laparoscopic procedures. Take four-port approach for laparoscopic procedure at the abdominal side. Make a 2 cm circular incision at the upper edge of the umbilicus. After establishing the pneumoperitoneum via the 10-mm camera port. Under laparoscopic visualization, 12-mm, 10-mm, and 5-mm ports were sequentially inserted via subumbilical two-finger-breadth incisions alongside the left and right rectus abdominis muscles and at the left retroperitoneal point, respectively, followed by insertion of operative instruments.
After exploring the abdominal and pelvic cavities to rule out other pathologies, use an ultrasonic scalpel to dissect adhesions between the omentum and abdominal wall/pelvic floor. The omentum was retracted cephalad toward the ileum and colon to fully expose the bladder, vaginal stump, and other pelvic structures. With assistance from gynecological forceps, use the ultrasonic scalpel to thoroughly dissect the space between the posterior bladder wall and the anterior vaginal stump, maximizing exposure and dissection of the fistula tract. The perineal assistant operates the cystoscope irrigation system to moderately distend the bladder. Localize the fistula orifice and tract using the cystoscope light source and the ureteral stent placed within the tract. Make a longitudinal incision through the posterior bladder wall to the fistula orifice. After aspirating all pelvic fluid, visually examine the fistula orifice and bilateral ureteral positions. Incise the fistula tract longitudinally, remove the positioned ureteral stent, and use tissue scissors to sharply excise necrotic and scar tissue surrounding the fistula orifice and tract. Scar tissue is excised. The vaginal stump anterior wall fistula opening is closed with 3-0 barbed sutures using a transverse continuous suture. The bladder posterior wall incision is then closed with 3-0 barbed sutures using a longitudinal continuous lockstitch full-thickness closure, ensuring the bladder posterior wall suture plane does not align with the vaginal wall suture plane. The assistant used a cystoscope to instill fluid and moderately distend the bladder. Under cystoscopic visualization, the integrity of the posterior bladder wall sutures and the absence of ureteral injury were assessed. Laparoscopic confirmation revealed no leakage at the posterior bladder wall suture site. Subsequently, the ureteral stents placed in both ureters were removed under cystoscopic guidance. Under laparoscopy, a 5 cm wide pedicled omental flap was dissected and tension-free retracted to cover the fistula opening in the vesicovaginal space, secured with 3-0 absorbable sutures. The pelvic cavity was irrigated with saline, and a pelvic drainage tube was placed. Retain an 18 Fr urinary catheter in the bladder for drainage. Remove the povidone-iodine gauze packplaced in the vagina and inserte a new povidone-iodine gauze pack. Surgery completed.
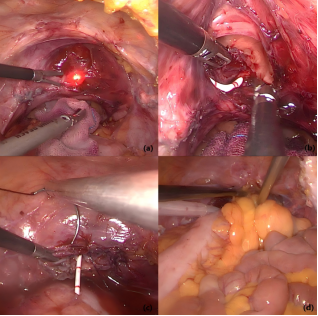
Figure 4. Surgical procedure. (a) Cystoscope light location. (b) Section of the bladder and ureteral stent location. (c) Closure of the bladder incision and vaginal fistula opening. (d) Dissect pedicled omental flap to cover the fistula opening in the vesicovaginal space.
3. Results
All 6 patients underwent successful surgery without any conversion to open procedures, and no complications such as intraoperative ureteral injury occurred. Operative time was 263.5±49.6 min. Intraoperative blood loss was 35.0±20.7 ml. Hospital stay was 15.5±5.4 days. Pelvic drainage tube removed after 2.5±0.5 days. Indwelling urinary catheter duration 16.7±2.7 days. No urinary leakage occurred after catheter removal. During follow-up ranging from 3 to 12 months, none of the 6 patients experienced postoperative complications such as urinary leakage or urinary tract infections. Postoperative quality of life showed significant improvement.
4. Discussion
In recent years, with advances in diagnostic and therapeutic techniques in obstetrics and gynecology and urology, along with increased surgical rates, iatrogenic injuries from gynecologic surgeries and pelvic malignancy radiotherapy have become primary causes of vesicovaginal fistula
[9]
Malik MA, Sohail M, Malik MT, Khalid N, Akram A. Changing trends in the etiology and management of vesicovaginal fistula. Int J Urol. 2018; 25(1): 25-29.
. Persistent urinary leakage severely impacts the quality of life for VVF patients, necessitating meticulous intraoperative techniques and prompt postoperative detection and repair of VVF.
The success of VVF repair depends on various factors, including fistula size, location, duration, severity, surrounding tissue quality, clinical experience, and surgical technique
[10]
Bragayrac LA, Azhar RA, Fernandez G, et al. Robotic repair of vesicovaginal fistulae with the transperitoneal-transvaginal approach: a case series. Int Braz J Urol. 2014; 40(6): 810-815.
. For early-detected simple vesicovaginal fistulas with an opening <3 mm, conservative management involving indwelling catheterization for 3 to 4 weeks
[11]
Alan J, Louis R, Andrew C, et a1. Campbell-Walsh Urology. 9th ed. Philadelphia: Saunders, 2007: 2322- 2359.
[11]
, alongside antibiotics for infection prevention may be considered. However, most VVF patients fail to respond to conservative management and require surgical intervention
[6]
Oakley SH, Brown HW, Greer JA, et al. Management of vesicovaginal fistulae: a multicenter analysis from the Fellows' Pelvic Research Network. Female Pelvic Med Reconstr Surg. 2014; 20(1): 7-13.
. The optimal timing for fistula repair remains controversial, with no definitive data on the most appropriate time for VVF repair. Typically, fistula formation and resolution of surrounding tissue inflammation, infection, and healing of necrotic tissue require 2 to 3 months
[12]
Rajaian S, Pragatheeswarane M, Panda A. Vesicovaginal fistula: Review and recent trends. Indian J Urol. 2019; 35(4): 250-258.
. Therefore, our research group elects to perform VVF repair 3 months after the onset of vaginal leakage. For VVFs occurring after radiotherapy, repair is postponed until 6 months post-treatment
[13]
Pushkar DY, Dyakov VV, Kasyan GR. Management of radiation-induced vesicovaginal fistula. Eur Urol. 2009; 55(1): 131-137.
. By this time, inflammation around the fistula opening is adequately controlled, and the fistula tract is fully formed, enhancing surgical success and reducing postoperative complications.
Surgical approaches for VVF repair include transvaginal, transvesical, and transabdominal approaches. The transvaginal approach is suitable for simple VVFs with few fistula openings, low location, and distance from the ureteral orifice. Conversely, the transabdominal approach is recommended for high-positioned or complex VVFs involving the trigone region, requiring ureteral reimplantation, or where vaginal access to the fistula tract and orifice is difficult
[14]
Chinthakanan O, Sirisreetreerux P, Saraluck A. Vesicovaginal Fistulas: Prevalence, Impact, and Management Challenges. Medicina (Kaunas). 2023; 59(11): 1947.
. With advances in minimally invasive surgical techniques, laparoscopic and robot-assisted laparoscopic approaches have been extensively adopted in urological and gynecological surgeries. Their efficacy has been demonstrated to be comparable to or even superior to open surgery
[15]
Abdel-Karim A, Elmissiry M, Moussa A, et al. Laparoscopic repair of female genitourinary fistulae: 10-year single-center experience. Int Urogynecol J. 2020; 31(7): 1357-1362.
Wang S, Zhang Y, Chen Z, et al. Laparoscopic distal gastrectomy demonstrates acceptable outcomes regarding complications compared to open surgery for gastric cancer patients with pylorus outlet obstruction. Front Oncol. 2023; 13: 1169454.
Zeng X, Li C, Yu M, et al. Laparoscopic versus open surgery for rectal neuroendocrine tumors: a multicenter real-world study. BMC Cancer. 2024; 24(1): 956.
Zhou X, Wei S, Shao Q, et al. Laparoscopic vs. open procedure for intermediate‑ and high‑risk endometrial cancer: a minimum 4-year follow-up analysis. BMC Cancer. 2022; 22(1): 1203.
Lecoanet P, Madanelo M, Tricard T, et al. Robot-assisted vesicovaginal fistula repair: comparison of the extravesical and transvesical techniques. Int Urogynecol J. 2023; 34(10): 2479-2485.
. When applied to VVF repair, laparoscopy magnifies the surgical field, provides clear visualization of anatomical layers, enables precise dissection of the fistula tract, and facilitates meticulous cutting and effective suturing. This significantly reduces intraoperative bleeding and collateral tissue damage while promoting postoperative recovery. Due to its satisfactory surgical outcomes, laparoscopic VVF repair has become the preferred technique for VVF reconstruction among an increasing number of urologists
[21]
Gözen AS, Teber D, Canda AE, Rassweiler J. Transperitoneal laparoscopic repair of iatrogenic vesicovaginal fistulas: Heilbronn experience and review of the literature. J Endourol. 2009; 23(3): 475-479.
. In this report, all 6 patients developed fistulas following hysterectomy or adjuvant radiotherapy. Due to high fistula locations or placement within the trigone region, vaginal access was impractical, necessitating transabdominal repair in all cases.
Traditional laparoscopic VVF repair typically involves locating and mapping the fistula under the lithotomy position during cystoscopy. The patient is then repositioned to supine or Trendelenburg posistion. After re-sterilization and draping, a pneumoperitoneum is established, followed by laparoscopic fistula repair. Our research team employs a combined laparoscopic and cystoscopic approach for VVF repair under a single position. Utilizing a modified lithotomy position with a 25° Trendelenburg tilt, we perform once sterilization and draping. Under cystoscopic guidance, we locate the intravesical fistula tract and place ureteral stents. The cystoscope's light source aids in fistula localization, while its irrigation system facilitates bladder distension and incision. Subsequently, laparoscopic techniques were used to repair the vesicovaginal fistula without changing the patient's position. Compared to conventional laparoscopic approaches, this combined approach enables faster and safer fistula localization, reduces the risk of adjacent tissue injury during bladder incision, minimizes surgical steps, shortens operative time, and decreases intraoperative blood loss.
Additionally, routine placement of ureteral stents in both ureters and the fistula tract during surgery effectively protects the ureters while facilitating precise localization of the fistula and target resection areas. During excision of the fistula tract and surrounding scar and necrotic tissue, sharp tissue shears are used instead of ultrasonic scalpels or electrocautery hooks to avoid thermal injury-related risks of poor fistula healing. Trim the margins to ensure adequate vascularity and enable tension-free suturing. During closure, perform transverse suturing on the vaginal stump and longitudinal suturing on the bladder wall fistula opening, positioning them on different planes to reduce postoperative urinary leakage. Layered suturing of the bladder and vaginal stump, along with tension-free bladder closure, are critical for surgical success.
After layered suturing of the bladder and vagina, appropriate graft tissues may be selected to fill the space between the bladder and vaginal fistula orifice. Examples include pedicled omentum or peritoneum. These graft tissues not only enhance blood supply between the fistula orifices but also absorb inflammatory exudate through their lymphatic system, thereby reducing the risk of postoperative infection and urinary leakage. The most commonly used patch currently is the omentum, which offers a large surface area, rich blood supply, and strong capacity for absorbing inflammatory exudate. After fibrosis of its fatty tissue, it adheres closely to the fistula wall, and its growth factors stimulate wound growth, promoting fistula healing
[22]
Sharma SK, Bapna BC, Gupta CL, et al. Pedicled omental graft in repair of large, difficult vesicovaginal fistulae. Int J Gynaecol Obstet. 1980; 17(6): 556-559.
. In this report, all 6 patients routinely received pedicled omentum coverage between the bladder and vaginal fistula orifices, with all surgeries successful.
However, this study has certain limitations. First, there is a risk of contamination between the intraoperative perineal cystoscope and the laparoscopic side, requiring close coordination between the primary surgeon and assistant to maintain aseptic principles and avoid interference during procedures. Second, the study included a small number of patients and was retrospective in nature. Therefore, future research should incorporate larger sample sizes and conduct long-term follow-up to validate efficacy, with plans for corresponding controlled studies.
5. Conclusions
In summary, performing transvaginal vesicovaginal fistula repair via combined cystoscopy and laparoscopy in a single position avoids multiple changes in surgical positioning. This approach offers advantages such as simplified technique, shorter operative time, minimal trauma, and reduced blood loss, making it a safe and effective therapeutic approach for VVF.
Abbreviations
VVF
Vesicovaginal Fistula
Author Contributions
Fengmeng Ou: Data curation, Formal Analysis, Methodology, Software, Visualization, Validation, Writing – original draft, Writing – review & editing
Guikang Wang: Data curation, Investigation, Methodology, Software
Jingwen Huang: Data curation, Investigation, Methodology
Adler AJ, Ronsmans C, Calvert C, Filippi V. Estimating the prevalence of obstetric fistula: a systematic review and meta-analysis. BMC Pregnancy Childbirth. 2013; 13: 246.
Duong TH, Taylor DP, Meeks GR. A multicenter study of vesicovaginal fistula following incidental cystotomy during benign hysterectomies. Int Urogynecol J. 2011; 22(8): 975-979.
Oakley SH, Brown HW, Greer JA, et al. Management of vesicovaginal fistulae: a multicenter analysis from the Fellows' Pelvic Research Network. Female Pelvic Med Reconstr Surg. 2014; 20(1): 7-13.
Nesrallah LJ, Srougi M, Gittes RF. The O'Conor technique: the gold standard for supratrigonal vesicovaginal fistula repair. J Urol. 1999; 161(2): 566-568.
Malik MA, Sohail M, Malik MT, Khalid N, Akram A. Changing trends in the etiology and management of vesicovaginal fistula. Int J Urol. 2018; 25(1): 25-29.
Bragayrac LA, Azhar RA, Fernandez G, et al. Robotic repair of vesicovaginal fistulae with the transperitoneal-transvaginal approach: a case series. Int Braz J Urol. 2014; 40(6): 810-815.
Abdel-Karim A, Elmissiry M, Moussa A, et al. Laparoscopic repair of female genitourinary fistulae: 10-year single-center experience. Int Urogynecol J. 2020; 31(7): 1357-1362.
Wang S, Zhang Y, Chen Z, et al. Laparoscopic distal gastrectomy demonstrates acceptable outcomes regarding complications compared to open surgery for gastric cancer patients with pylorus outlet obstruction. Front Oncol. 2023; 13: 1169454.
Zeng X, Li C, Yu M, et al. Laparoscopic versus open surgery for rectal neuroendocrine tumors: a multicenter real-world study. BMC Cancer. 2024; 24(1): 956.
Zhou X, Wei S, Shao Q, et al. Laparoscopic vs. open procedure for intermediate‑ and high‑risk endometrial cancer: a minimum 4-year follow-up analysis. BMC Cancer. 2022; 22(1): 1203.
Lecoanet P, Madanelo M, Tricard T, et al. Robot-assisted vesicovaginal fistula repair: comparison of the extravesical and transvesical techniques. Int Urogynecol J. 2023; 34(10): 2479-2485.
Ou, F., Wang, G., Huang, J., Pan, B. (2026). Clinical Application of Combined Cystoscopy and Laparoscopy for Vesicovaginal Fistula Repair in a Single Position: Six Cases Report and Experience. International Journal of Clinical Urology, 10(1), 42-47. https://doi.org/10.11648/j.ijcu.20261001.18
Ou, F.; Wang, G.; Huang, J.; Pan, B. Clinical Application of Combined Cystoscopy and Laparoscopy for Vesicovaginal Fistula Repair in a Single Position: Six Cases Report and Experience. Int. J. Clin. Urol.2026, 10(1), 42-47. doi: 10.11648/j.ijcu.20261001.18
Ou F, Wang G, Huang J, Pan B. Clinical Application of Combined Cystoscopy and Laparoscopy for Vesicovaginal Fistula Repair in a Single Position: Six Cases Report and Experience. Int J Clin Urol. 2026;10(1):42-47. doi: 10.11648/j.ijcu.20261001.18
@article{10.11648/j.ijcu.20261001.18,
author = {Fengmeng Ou and Guikang Wang and Jingwen Huang and Bin Pan},
title = {Clinical Application of Combined Cystoscopy and Laparoscopy for Vesicovaginal Fistula Repair in a Single Position: Six Cases Report and Experience},
journal = {International Journal of Clinical Urology},
volume = {10},
number = {1},
pages = {42-47},
doi = {10.11648/j.ijcu.20261001.18},
url = {https://doi.org/10.11648/j.ijcu.20261001.18},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcu.20261001.18},
abstract = {Objective: To evaluate the clinical efficacy of combined cystoscopy and laparoscopy for vesicovaginal fistula repair in a single position. Methods: A retrospective analysis was conducted on the clinical data of 6 patients with vesicovaginal fistula treated in the Department of Urology, The First Affiliated Hospital of Jinan University from August 2017 to November 2023. All patients underwent a single-position cystoscopy combined with laparoscopic vesicovaginal fistula repair. Intraoperatively, the fistula was localized transurethrally via cystoscopy, and place ureteral stents. Simultaneously, laparoscopic repair of the fistula was performed via abdominal approach. Recording Surgical duration, intraoperative blood loss, length of hospital stay, intraoperative complications and postoperative complications. Results: All 6 patients underwent successful repair without conversion to open surgery. Operative time was 263.5±49.6 min, intraoperative blood loss was 35.0±20.7 ml, hospital stay was 15.5±5.4 days. At follow-up ranging from 3 to 12 months, no patients developed complications such as urinary leakage, and postoperative quality of life showed significant improvement. Conclusion: Combined cystoscopy and laparoscopy for vesicovaginal fistula repair in a single position avoids multiple repositioning, offering advantages such as simplified technique, short operative time, minimal trauma, and reducedloss blood. This approach represents a safe and effective therapeutic modality.},
year = {2026}
}
TY - JOUR
T1 - Clinical Application of Combined Cystoscopy and Laparoscopy for Vesicovaginal Fistula Repair in a Single Position: Six Cases Report and Experience
AU - Fengmeng Ou
AU - Guikang Wang
AU - Jingwen Huang
AU - Bin Pan
Y1 - 2026/03/23
PY - 2026
N1 - https://doi.org/10.11648/j.ijcu.20261001.18
DO - 10.11648/j.ijcu.20261001.18
T2 - International Journal of Clinical Urology
JF - International Journal of Clinical Urology
JO - International Journal of Clinical Urology
SP - 42
EP - 47
PB - Science Publishing Group
SN - 2640-1355
UR - https://doi.org/10.11648/j.ijcu.20261001.18
AB - Objective: To evaluate the clinical efficacy of combined cystoscopy and laparoscopy for vesicovaginal fistula repair in a single position. Methods: A retrospective analysis was conducted on the clinical data of 6 patients with vesicovaginal fistula treated in the Department of Urology, The First Affiliated Hospital of Jinan University from August 2017 to November 2023. All patients underwent a single-position cystoscopy combined with laparoscopic vesicovaginal fistula repair. Intraoperatively, the fistula was localized transurethrally via cystoscopy, and place ureteral stents. Simultaneously, laparoscopic repair of the fistula was performed via abdominal approach. Recording Surgical duration, intraoperative blood loss, length of hospital stay, intraoperative complications and postoperative complications. Results: All 6 patients underwent successful repair without conversion to open surgery. Operative time was 263.5±49.6 min, intraoperative blood loss was 35.0±20.7 ml, hospital stay was 15.5±5.4 days. At follow-up ranging from 3 to 12 months, no patients developed complications such as urinary leakage, and postoperative quality of life showed significant improvement. Conclusion: Combined cystoscopy and laparoscopy for vesicovaginal fistula repair in a single position avoids multiple repositioning, offering advantages such as simplified technique, short operative time, minimal trauma, and reducedloss blood. This approach represents a safe and effective therapeutic modality.
VL - 10
IS - 1
ER -
Ou, F., Wang, G., Huang, J., Pan, B. (2026). Clinical Application of Combined Cystoscopy and Laparoscopy for Vesicovaginal Fistula Repair in a Single Position: Six Cases Report and Experience. International Journal of Clinical Urology, 10(1), 42-47. https://doi.org/10.11648/j.ijcu.20261001.18
Ou, F.; Wang, G.; Huang, J.; Pan, B. Clinical Application of Combined Cystoscopy and Laparoscopy for Vesicovaginal Fistula Repair in a Single Position: Six Cases Report and Experience. Int. J. Clin. Urol.2026, 10(1), 42-47. doi: 10.11648/j.ijcu.20261001.18
Ou F, Wang G, Huang J, Pan B. Clinical Application of Combined Cystoscopy and Laparoscopy for Vesicovaginal Fistula Repair in a Single Position: Six Cases Report and Experience. Int J Clin Urol. 2026;10(1):42-47. doi: 10.11648/j.ijcu.20261001.18
@article{10.11648/j.ijcu.20261001.18,
author = {Fengmeng Ou and Guikang Wang and Jingwen Huang and Bin Pan},
title = {Clinical Application of Combined Cystoscopy and Laparoscopy for Vesicovaginal Fistula Repair in a Single Position: Six Cases Report and Experience},
journal = {International Journal of Clinical Urology},
volume = {10},
number = {1},
pages = {42-47},
doi = {10.11648/j.ijcu.20261001.18},
url = {https://doi.org/10.11648/j.ijcu.20261001.18},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcu.20261001.18},
abstract = {Objective: To evaluate the clinical efficacy of combined cystoscopy and laparoscopy for vesicovaginal fistula repair in a single position. Methods: A retrospective analysis was conducted on the clinical data of 6 patients with vesicovaginal fistula treated in the Department of Urology, The First Affiliated Hospital of Jinan University from August 2017 to November 2023. All patients underwent a single-position cystoscopy combined with laparoscopic vesicovaginal fistula repair. Intraoperatively, the fistula was localized transurethrally via cystoscopy, and place ureteral stents. Simultaneously, laparoscopic repair of the fistula was performed via abdominal approach. Recording Surgical duration, intraoperative blood loss, length of hospital stay, intraoperative complications and postoperative complications. Results: All 6 patients underwent successful repair without conversion to open surgery. Operative time was 263.5±49.6 min, intraoperative blood loss was 35.0±20.7 ml, hospital stay was 15.5±5.4 days. At follow-up ranging from 3 to 12 months, no patients developed complications such as urinary leakage, and postoperative quality of life showed significant improvement. Conclusion: Combined cystoscopy and laparoscopy for vesicovaginal fistula repair in a single position avoids multiple repositioning, offering advantages such as simplified technique, short operative time, minimal trauma, and reducedloss blood. This approach represents a safe and effective therapeutic modality.},
year = {2026}
}
TY - JOUR
T1 - Clinical Application of Combined Cystoscopy and Laparoscopy for Vesicovaginal Fistula Repair in a Single Position: Six Cases Report and Experience
AU - Fengmeng Ou
AU - Guikang Wang
AU - Jingwen Huang
AU - Bin Pan
Y1 - 2026/03/23
PY - 2026
N1 - https://doi.org/10.11648/j.ijcu.20261001.18
DO - 10.11648/j.ijcu.20261001.18
T2 - International Journal of Clinical Urology
JF - International Journal of Clinical Urology
JO - International Journal of Clinical Urology
SP - 42
EP - 47
PB - Science Publishing Group
SN - 2640-1355
UR - https://doi.org/10.11648/j.ijcu.20261001.18
AB - Objective: To evaluate the clinical efficacy of combined cystoscopy and laparoscopy for vesicovaginal fistula repair in a single position. Methods: A retrospective analysis was conducted on the clinical data of 6 patients with vesicovaginal fistula treated in the Department of Urology, The First Affiliated Hospital of Jinan University from August 2017 to November 2023. All patients underwent a single-position cystoscopy combined with laparoscopic vesicovaginal fistula repair. Intraoperatively, the fistula was localized transurethrally via cystoscopy, and place ureteral stents. Simultaneously, laparoscopic repair of the fistula was performed via abdominal approach. Recording Surgical duration, intraoperative blood loss, length of hospital stay, intraoperative complications and postoperative complications. Results: All 6 patients underwent successful repair without conversion to open surgery. Operative time was 263.5±49.6 min, intraoperative blood loss was 35.0±20.7 ml, hospital stay was 15.5±5.4 days. At follow-up ranging from 3 to 12 months, no patients developed complications such as urinary leakage, and postoperative quality of life showed significant improvement. Conclusion: Combined cystoscopy and laparoscopy for vesicovaginal fistula repair in a single position avoids multiple repositioning, offering advantages such as simplified technique, short operative time, minimal trauma, and reducedloss blood. This approach represents a safe and effective therapeutic modality.
VL - 10
IS - 1
ER -